Lessico
Herpes zoster
Zona
Fuoco di Sant'Antonio
![]()
Etimologia:
malattia che striscia a cintura.
- Latino herpes, gen.
herpetis, dal geco hérpës, gen. hérpëtos, derivato di
hérpein ‘strisciare’. - Latino nominativo zoster,
riproduzione del greco zřstër gen. zřstęros ‘cintura’ (l’italiano zona viene dal greco zřnë, lett.
‘cintura’) di cui si servě Teofrasto![]() per indicare una specie di alga.
per indicare una specie di alga.
Malattia a
eziologia virale (virus neurodermotropo), nella quale vengono colpiti gangli
spinali e radici posteriori di nervi spinali, nota anche come "fuoco di Sant'Antonio![]() ".
".
L'odierno
fuoco di Sant'Antonio di origine virale non č da confondere con il
termine omonimo usato nei secoli passati, che spesso indicava l'ergotismo,
una sindrome determinata dalla segale cornuta![]() (il fungo Claviceps purpurea che attacca la segale e altri cereali),
sindrome che era anche detta "fuoco persiano
(il fungo Claviceps purpurea che attacca la segale e altri cereali),
sindrome che era anche detta "fuoco persiano![]() ".
".
Per l'herpes zoster di origine virale vi sono possibilitŕ di contagio crociato con la varicella, ma puň manifestarsi spontaneamente o anche nel corso di intossicazioni (da ossido di carbonio, arsenico, bismuto, ecc.), infezioni acute e croniche, traumi cranici, ecc. Conferisce immunitŕ.
I sintomi compaiono qualche giorno prima con dolori, bruciore, talora febbre, disturbi gastrointestinali; poi, sempre monolateralmente, lungo il decorso di uno o piů tronchi nervosi vicini, si manifestano placche eritemato-edematose che possono rimanere a questo stadio (herpes zoster abortivo) o, piů di frequente, si ricoprono di gruppi di vescicole tese a contenuto limpido, poi torbido (talora emorragico), accompagnate da parestesie o forti dolori nevralgici, persistenti specie nei vecchi anche dopo la risoluzione della dermatosi.
Coesiste precoce adenopatia satellite. La durata varia da una a quattro settimane, poi avviene l'afflosciamento e l'essiccamento delle vescicole con esiti cicatriziali, spesso pigmentari, permanenti.
Le sedi piů frequenti sono: la cervicale, la cervico-brachiale, l'intercostale, la toraco-addominale, la regione della branca oftalmica del trigemino, talora con lesioni corneali e paralisi dell'oculomotore. Per fortuna queste lesioni corneali e la paralisi dell'oculomotore non si sono presentate in Elio Corti (non sappiamo se per intercessione di Sant'Antonio) colpito appunto nel novembre 2007 da herpes zoster a carico della branca oftalmica del trigemino.

Elio
Corti - 13 novembre 2007
Herpes zoster con interessamento del ramo sopraorbitale
della branca oftalmica del trigemino destro
accompagnato da linfoadenopatia satellite sottomandibolare.
Foto di Luca Pasero![]()



Herpes
zoster
Shingles
Herpes zoster, colloquially known as shingles, is the reactivation (from the nerve cell body in the sensory ganglion of a segment of the spinal cord) of varicella zoster virus (VZV, primary infection of which leads to chickenpox), one of the Herpesviridae group, leading to a crop of painful blisters over the area of a dermatome. In Italy and in Malta, it is sometimes referred to as "St. Anthony's fire", although that name usually refers to ergotism. Shingles, or herpes zoster, is a neurological disease, affecting the nervous system with or without the appearance of a rash on the skin.
Treatment is generally with antiviral drugs such as acyclovir (Zovirax), or prodrugs such as famciclovir (Famvir), or valacyclovir (Valtrex). For the antiviral drugs to be most effective, patients should begin taking them as soon as possible after the appearance of the rash, within 12 to 72 hours for maximum efficacy.
Signs and symptoms
The earliest symptoms (constituting the prodrome) of shingles include headache, sensitivity to light, fever, and malaise, all of which may, within one to several days, be followed by itching, tingling, and pain which may be extreme in the distribution of the affected nerve, where the rash will later develop. This pain can be characterized as stinging, tingling, aching, numbing, or throbbing, and can be pronounced with quick stabs of intensity. During this phase, herpes zoster is frequently misdiagnosed as other diseases with similar symptoms, including heart attacks and renal colic. Some patients may have these symptoms without developing the characteristic rash. This situation, known as "zoster sine herpete," can delay diagnosis and treatment.
The initial phase is followed by development of the characteristic skin rashes of herpes zoster. The skin lesions begin as a rash, similar to hives, that follows a distribution near dermatomes, commonly occurring in a strip or belt-like pattern. The rash evolves into vesicles or small blisters filled with serous fluid. The vesicles are generally painful, and their development is often associated with the occurrence of anxiety and further flu-like symptoms, such as fever, tiredness, and generalized pain. The vesicles eventually become hemorrhagic (filled with blood), and crust over within seven to 10 days. As the crusts fall off, patients are commonly left with scarring and pigmented skin.
Shingles cannot be passed from one person to another. However, the virus that causes shingles, VZV, can be spread from a person with active shingles to a person who has never had chickenpox through direct contact with the rash. The person exposed would then develop chickenpox, not shingles. The virus is not spread through sneezing, coughing or casual contact. A person with shingles can spread the disease when the rash is in the blister-phase. Once the rash has developed crusts, the person is no longer contagious. A person is not infectious before blisters appear or with post-herpetic neuralgia (pain after the rash is gone).
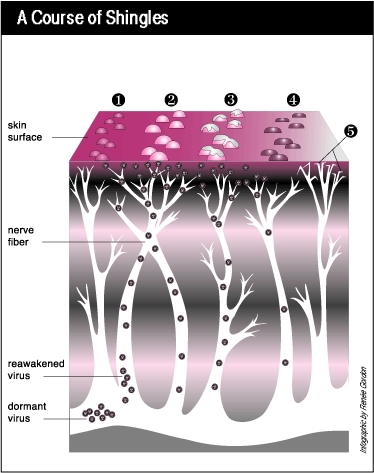
Chickenpox virus can remain dormant for decades, and does so inside the ganglion of the spinal cord. As the virus is reactivated it spreads down peripheral nerve fibers and produces intense pain. The blisters therefore only affect one area of the body and do not cross the midline. They are most common on the torso, but can also appear on the face (where they are potentially hazardous to vision) or other parts of the body.
Causes
Shingles can only arise in individuals who have had previous exposure to chicken pox (varicella zoster). Individuals develop shingles for many different reasons, most of which are thought to be a result of events which depress the immune system, such as aging, severe emotional stress, severe illness, immunosuppression or long-term use of corticosteroids. However, the cellular and immunological events that lead to reactivation are poorly understood. There have been recorded cases of outbreaks occurring due to unmanaged stress or other stresses to the skin such as pinching in more sensitive areas of the skin (nipples, ears, and underarms), scratching, or biting.
Pathophysiology
The causative agent for herpes zoster is varicella zoster virus (VZV). Most people are infected with this virus as a child, as it causes chickenpox. The body eliminates the virus from the system, but it remains dormant in the ganglia adjacent to the spinal cord (called the dorsal root ganglion) or the ganglion semilunare (ganglion Gasseri) in the cranial base.
Generally, the immune system suppresses reactivation of the virus. In the elderly, whose immune response generally tends to deteriorate, as well as in those patients whose immune system is being suppressed, this process fails. (Some researchers speculate that sunburn and other, unrelated stresses that can affect the immune system may also lead to viral reactivation.) The virus starts replicating in the nerve cells, and newly formed viruses are carried down the axons to the area of skin served by that ganglion (a dermatome). Here, the virus causes local inflammation in the skin, with the formation of blisters. The pain characteristic of herpes zoster is thought to be due to irritation of the sensory nerve fibers in which the virus reproduces.
Diagnosis
The diagnosis is visual; very few other diseases mimic herpes zoster, especially in the localization of the rash, which is otherwise quite similar in appearance and initial effect to that of poison oak or poison ivy (although it may not be accompanied by the intense itching so characteristic of those rashes).
In case of doubt, diagnostic tests can be performed. Such lab tests may be necessary because, depending on the affected sensory nerve, the pain that is experienced before the onset of the rash may be misdiagnosed as pleurisy, myocardial infarction, appendicitis, cholelithiasis, or a migraine headache. Fluid from a blister may be taken so the cells can be analyzed in a medical laboratory. While looking at the cells obtained from the blister, those infected with the herpes virus will appear very large and contain many dark nuclei. A physician can also take a viral culture of a fresh lesion, or perform a microscopic examination of the blister base called a Tzanck preparation. In a complete blood count there may be an elevated number of white blood cells, which is an indirect sign of infection. There may also be a rise in the antibody to the virus, which would also give indication of the virus’ reactivation.
Treatment
Currently, there is no cure available for Herpes zoster, nor a treatment to effectively eliminate the virus from the body. However, there are some treatments that can mitigate the length of the disease and alleviate certain side effects.
Antiviral drugs
Acyclovir (an antiviral drug) inhibits replication of the viral DNA, and is used both as prophylaxis (e.g., in patients with AIDS) and as therapy for herpes zoster. Other antivirals are valacyclovir and famciclovir. During the acute phase, oral acyclovir should be given. Use of acylovir is most effective in moderating the progress of the symptoms, and in preventing post-herpetic neuralgia, if started within 24 to 72 hours of the onset of symptoms, so medical care should be obtained as soon as the condition is recognized. Immunocompromised patients may respond best to intravenous acyclovir. In patients who are at high risk for recurrences, an oral dose of acyclovir, taken twice daily, is usually effective. It is also reported that the amino acid lysine inhibits the replication of herpes zoster.
Other drugs
Cimetidine, a common component of over-the-counter heartburn medication, has been shown to lessen the severity of herpes zoster outbreaks in several different instances. This usage is considered an off-label use of the drug. In addition, cimetidine and probenecid have been shown to reduce the renal clearance of aciclovir. The study showed these compounds reduce the rate, but not the extent, at which valaciclovir is converted into aciclovir. Renal clearance of aciclovir was reduced by approximately 24% and 33% respectively. In addition, respective increases in the peak plasma concentration of acyclovir of 8% and 22% were observed. The authors concluded that these effects were "not expected to have clinical consequences regarding the safety of valaciclovir". Due to the tendency of aciclovir to precipitate in renal tubules, combining these drugs should only occur under the supervision of a physician.
Complementary therapies
Digestive Enzymes are available on script and in some over the counter preparations. Before the availability of antivirals, oral pancreatic enzyme therapy in shingles was used in some countries and later subjected to clinical and scientific research. A large scale multi-centre clinical study, using an oral preparation of such enzymes, has shown promising results. The results of another clinical study support the concept that oral enzyme therapy is beneficial in diseases characterized in part by TGF-beta overproduction that included shingles patients. [15] TGF-B has also been found higher in instances of VZV.
Prognosis
The rash and pain usually subside within 3 to 5 weeks. Many patients develop a painful condition called postherpetic neuralgia, which is often difficult to manage. In some patients, herpes zoster can reactivate subclinically, with pain in a dermatomal distribution without rash. This condition is known as zoster sine herpete, and may be more complicated, affecting multiple levels of the nervous system and causing multiple cranial neuropathies, polyneuritis, myelitis, or aseptic meningitis. Sometimes serious effects including partial facial paralysis (usually temporary), ear damage, or encephalitis may occur. Shingles on the upper half of the face (the first branch of the trigeminal nerve) may result in eye damage and require urgent ophthalmological assessment. Ocular complications occur in approximately one half of patients with involvement of the ophthalmic division of the trigeminal nerve. These complications include mucopurulent conjunctivitis, episcleritis, keratitis and anterior uveitis. Cranial nerve palsies of the third, fourth and sixth cranial nerves may occur, affecting extraocular motility.
Since shingles is a reactivation of a virus contracted previously — often decades earlier — it cannot be induced by exposure to another person with shingles or chickenpox. Those with active blisters, however, can spread chickenpox to others who have never had that condition and who have not been vaccinated against it.
Prevention
Zostavax is a vaccine developed by Merck & Co. which has proven successful in preventing half the cases of herpes zoster in a study of 38,000 people who received the vaccine. The vaccine also reduced by two-thirds the number of cases of postherpetic neuralgia. However, prior to the vaccine, it has long been known that adults received natural immune boosting from contact with children infected with varicella. This helped to suppress the reactivation of herpes zoster. In Massachusetts, herpes zoster incidence increased 90%, from 2.77/1000 to 5.25/1000 in the period of increasing varicella vaccination 1999-2003. The effectiveness of the varicella vaccine itself is dependent on this exogenous (outside) boosting mechanism. Thus, as natural cases of varicella decline, so has the effectiveness of the vaccine.
The intake of micronutrients, including antioxidant vitamins, A, C, E and vitamin B, as well as fresh fruit, may reduce the risk of developing shingles. In one study, patients who consumed less than one serving of fruit a day had three times the risk as those who consumed over three servings per day. For those aged 60 or more, micronutrient and vegetable intake had a similar lowering of risk. A recent study evaluated the effects of two types of behavioral intervention, Tai Chi and health education, on healthy adults, who, after 16 weeks of the intervention, were vaccinated with VARIVAX, a live attenuated Oka/Merck Varicella zoster virus vaccine.
Epidemiology
Prior to implementation of the universal varicella vaccination program in the U.S., incidence of shingles increased with advancing age in association with a progressive decline in immunity to varicella-zoster virus. Shingles incidence is highest in persons who are over age 55, as well as in immunocompromised patients regardless of age group. The incidence rate of Herpes zoster in persons aged 65 or older is approximately 19 per 1000 individuals per year in the US. The incidence in whites of this age group is approximately 3.5 times higher than in hispanics. It can also be seen in immunocompetent individuals undergoing severe emotional stress.
![]()